Inverted Papilloma
• Rare, ~1% of urothelial neoplasms seen over a wide age range
• Cystoscopy shows small (<3 cm) solitary sessile lesion or may have a short stalk.
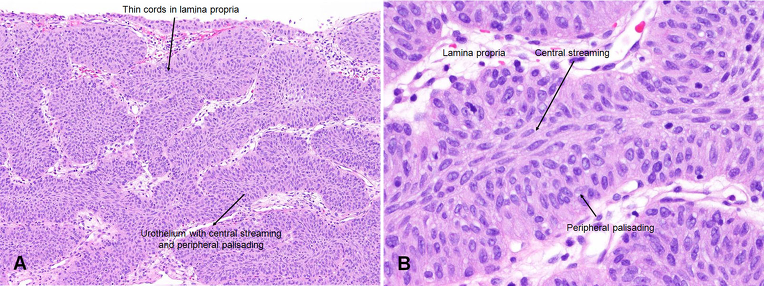
• Histology:
◦Urothelium invaginates into lamina propria (inverted).
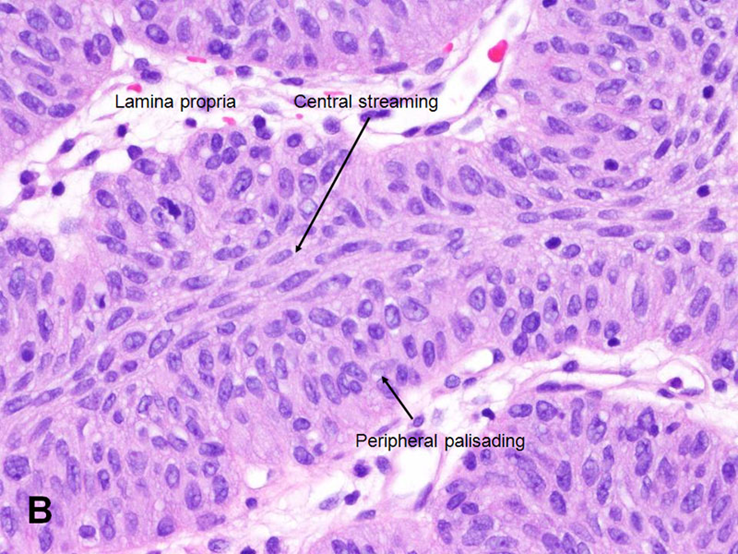
◦Characterized by cords or trabeculae with peripheral palisading of basal cells and central streaming cells.
◦Cords should be thin (a must, to distinguish from higher grade inverted urothelial neoplasms).
◦Bland cytology, but may have scattered degenerative atypia.
• Benign proliferative lesion (associated with chronic inflammation or bladder outlet obstruction)
• Can be located throughout the bladder but most commonly on the trigone, comprising less than 1% of all bladder tumors
• Inverted growth pattern (anastomosing islands of histologically and cytologically normal urothelial cells invaginating from the surface urothelium into the lamina propria but not into the muscularis propria)
• Behave in a benign fashion with only a 1% incidence of tumor recurrence. (Negligible recurrence rate (<1%))
• Occasionally, present with coexistent urothelial cancer elsewhere in the urinary system, occurring more commonly in the upper tract than the bladder
• The use of fluorescent in-situ hybridization (FISH) to evaluate chromosomal changes can distinguish between an inverted papilloma and a urothelial cancer with an inverted growth pattern (Jones et al, 2007).
• Transurethral resection is the treatment of choice.
Referrence
1. Campbell Urology
Chapter 80 : Urothelial Tumors of the Bladder
No comments:
Post a Comment